The Anterior Cruciate Ligament (ACL) is the main stabilizer of the knee joint for athletic pivotal activities. It is composed of two separate bundles, the anteromedial and the posterolateral. The intra-articular length of the ligament is between 28 and 31mm. The ACL has been described as a
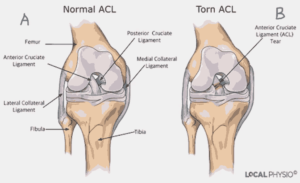
multifascicular structure originating on the antero-medial aspect of the tibia, with a sagittal and coronal oblique course towards the posterior aspect of the medial side of the lateral femoral condyle. (Figure 1).
The ACL’s main blood supply is derived from branches of the middle genicular artery. These form a network in the synovial membrane surrounding the ligament, with secondary contributions from the medial and lateral geniculate at the tibial insertion. The bony attachments are of less nutritional importance.
With the increase in sports participation worldwide, injury to the ACL has become one of the most common athletic injuries and it is the most reconstructed ligament in the human body. In the 1970s, the torn ACL was considered the beginning of a progressive deterioration of the knee that often ended an athlete’s career. However, with the improvement in arthroscopy and sports medicine, many athletes now routinely return to play as soon as four to six months after an injury.
Source of Image: Atlanta’s Resource for Orthopaedic Surgery. https://www.atlantaboneandjoint.com/acltear.html
Figure 1: Diagrammatic representation of Major Knee Ligaments. A – Normal ACL, B – Torn ACL
In a typical scenario, the patient describes a twisting injury to his knee, associated with a “popping” sensation in the knee. This is followed by immediate pain and swelling of the knee. Pain can range from minimal and transient to severe and long-lasting. It may be described as deep in the knee but is more often felt anterior on either side of the patellar tendon or laterally on the joint line. In about 80% of ACL injuries, individuals experience a popping, snapping, or tearing sensation. A rapid onset (usually within 3 hours) of swelling (hemarthrosis) is also seen in about eighty percent. Swelling is described as “a poor-man” MRI scan of the knee; in traumatic knee, a swelling is an indication of an underlying pathology. Weight-bearing leads to a feeling of the knee giving way or “just not feeling right.” The patient may indicate the feeling of the knee giving way with the “2-fist sign”. (Figure 2)

Picture source: National Orthopaedic Hospital, Dala, Kano, Nigeria
Figure 2: An athlete demonstrating the “2-fist sign” of his knee instability
When properly done, a physical examination can demonstrate all cases of complete ACL tears. The Lachman test is the most definitive and easily performed test for ACL tears. It is performed with the patient in the supine position. The knee is flexed to 30°, the femur is stabilized by the upper hand, and the tibia is pulled forward using the lower hand (Figure 3). The test is positive when the endpoint is soft. The main feeling is the lack of an endpoint to the anterior translation of the tibia. Comparing to the opposite side is important. Other clinical signs to demonstrate ACL tear include the anterior drawer test and pivot shift test. The pivot shift test is done with the patient lying on their back with the affected knee fully extended and the tibia internally rotated, the tester stresses the knee with a coupled valgus and internal rotation force and flexes the knee. An appreciable clunk felt around 30° of knee flexion indicates that the subluxated joint has reduced and indicates a complete ACL tear. Complete knee examinations are also done to rule out other associated injuries.


Picture source: National Orthopaedic Hospital, Dala, Kano, Nigeria
Figure 3: Demonstration of clinical signs in ACL injury diagnosis. (A) Anterior drawer test, (B) Lachman test.
Radiological examination of the knee should always start with plain radiographs. This will reveal ACL bony avulsions, significant osteochondral fractures, tibial plateau fractures, or segond fracture that is associated with ACL tears in about 75% of cases.
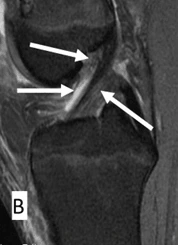
Magnetic Resonance Imaging (MRI) is very useful in diagnosing ACL injury. Though, the diagnosis of ACL rupture is clinical and a good physical examination by an experienced physician is more reliable than an MRI. However, in a few situations, magnetic resonance imaging (MRI) will change your management of an injury. It may be required to differentiate between a cyclops lesion of the ACL and a bucket handle tear of the meniscus. The sensitivity and specificity of an MRI in diagnosing ACL tears are 86% and 95% respectively. Other important tests for diagnosing an ACL tear in the operating room are examination under anaesthesia EUA and diagnostic arthroscopy (Figure 5).

Picture source: National Orthopaedic Hospital, Dala, Kano, Nigeria
Figure 4: Sagittal view of Knee MRI showing ACL. (A) Normal ACL, (B) Torn AC
L
Picture source: National Orthopaedic Hospital, Dala, Kano, Nigeria
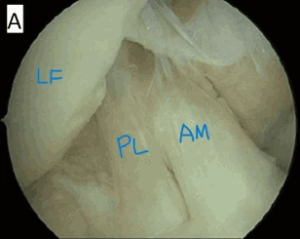
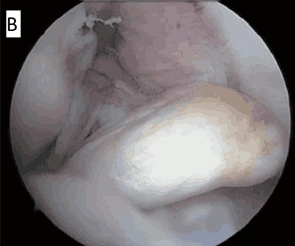
Figure 5: Arthroscopic anatomy of ACL. (A) Normal ACL, LF – Lateral femoral condyle, PL – Posterolateral bundle, AM – Anteromedial bundle. (B) Ruptured ACL
Once it has torn, attempts to surgically repair ACL tears are not successful. Consequently, better results are obtained if the ACL is surgically reconstructed with another tendon. The surgical procedure is mostly performed using arthroscopic techniques. Using one or two small incisions on the knee, the graft is taken from the patellar tendon, hamstring tendons or peroneus longus tendon, and a tunnel is drilled into both the tibia and femur. The graft is threaded across the knee, The graft is then secured in position, most commonly by “wedging” a screw (interference screw) between the side of the bone and the tunnel. Alternatively, the graft can be secured by other techniques — staples, sutures, buttons, etc. These fixation devices are usually left in place permanently.

Figure 6: Knee Arthroscopy being performed

Figure 7: Peroneus Longus Graft being harvested using a tendon stripper.

Figure 8: Peroneus Longus graft prepared for ACL Reconstruction.

Figure 9: ACL graft is fixed to the tibia tunnel with an absorbable interference screw.
Pictures Sources: National Orthopaedic Hospital Dala Kano

The Anterior Cruciate Ligament (ACL) is the main stabilizer of the knee joint for athletic pivotal activities. It is composed of two separate bundles, the anteromedial and the posterolateral. The intra-articular length of the ligament is between 28 and 31mm. The ACL has been described as a
multifascicular structure originating on the antero-medial aspect of the tibia, with a sagittal and coronal oblique course towards the posterior aspect of the medial side of the lateral femoral condyle. (Figure 1).
The ACL’s main blood supply is derived from branches of the middle genicular artery. These form a network in the synovial membrane surrounding the ligament, with secondary contributions from the medial and lateral geniculate at the tibial insertion. The bony attachments are of less nutritional importance.
With the increase in sports participation worldwide, injury to the ACL has become one of the most common athletic injuries and it is the most reconstructed ligament in the human body. In the 1970s, the torn ACL was considered the beginning of a progressive deterioration of the knee that often ended an athlete’s career. However, with the improvement in arthroscopy and sports medicine, many athletes now routinely return to play as soon as four to six months after an injury.
Source of Image: Atlanta’s Resource for Orthopaedic Surgery. https://www.atlantaboneandjoint.com/acltear.html
Figure 1: Diagrammatic representation of Major Knee Ligaments. A – Normal ACL, B – Torn ACL
1. Arojuraye SA, Salihu MN, Salahudeen A. Arthroscopic Anterior Cruciate Ligament Reconstruction Learning Curve: Analysis of Operating Time and Clinical Outcomes. J West Afr Coll Surg. 2024 Apr-Jun;14(2):208-211.
2. Alabi IA, Nkanta C, Okoh N, Arojuraye SA and Abbas AD. Functional Outcome of Arthroscopic Reconstruction of Chronic Anterior Cruciate ligament Rupture using Single-bundle Triple-weaved Hamstring Tendons in Northern Nigeria. International Journal of Orthopaedics Sciences 2020; 6(4): 533-538.
3. Leon S, Carol V. David S. Anterior Cruciate Ligament Injuries: Anatomy, Physiology, Biomechanics, and Management. Clin J Sport Med 2012; 22(4): 349 – 355.
4. Douglas WA, Peter RK. Anterior Cruciate Ligament Reconstruction. In: Douglas WJ. Master Techniques in Orthopaedic Surgery; Reconstructive knee Surgery. Lippincott Williams & Wilkins 2008; 3rd Ed, 3: 132 – 153
5. Shelbourne KD, Benner RW, Ringenberg JD, Gray T. Optimal management of posterior cruciate ligament injuries: current perspectives. Orthop Res Rev. 2017;9:13-22
6. Bolgla LA. Gender issues in ACL injury. In: Giangarra CE, Manske RC, eds. Clinical Orthopaedic Rehabilitation: A Team Approach. 4th ed. Philadelphia, PA: Elsevier; 2018:chap 49.
7. Brotzman SB. Anterior cruciate ligament injuries. In: Giangarra CE, Manske RC, eds. Clinical Orthopaedic Rehabilitation: A Team Approach. 4th ed. Philadelphia, PA: Elsevier; 2018:chap 47.
8. Cheung EC, McAllister DR, Petrigliano FA. Anterior cruciate ligament injuries. In: Miller MD, Thompson SR, eds. DeLee, Drez, & Miller’s Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 98.
9. Gokeler A, Dingenen B, Hewett TE. Rehabilitation and return to sport testing after anterior cruciate ligament reconstruction: where are we in 2022? Arthrosc Sports Med Rehabil. 2022;4(1):e77-e82.
10. Kalawadia JV, Guenther D, Irarrázaval S, Fu FH. Anatomy and biomechanics of the anterior cruciate ligament. In: Prodomos CC. The Anterior Cruciate Ligament: Reconstruction and Basic Science. 2nd ed. Philadelphia, PA: Elsevier; 201
8:chap 1.

Background
The Anterior Cruciate Ligament (ACL) is the main stabilizer of the knee joint for athletic pivotal activities. It is composed of two separate bundles, the anteromedial and the posterolateral. The intra-articular length of the ligament is between 28 and 31mm. The ACL has been described as a
multifascicular structure originating on the antero-medial aspect of the tibia, with a sagittal and coronal oblique course towards the posterior aspect of the medial side of the lateral femoral condyle. (Figure 1).
The ACL’s main blood supply is derived from branches of the middle genicular artery. These form a network in the synovial membrane surrounding the ligament, with secondary contributions from the medial and lateral geniculate at the tibial insertion. The bony attachments are of less nutritional importance.
With the increase in sports participation worldwide, injury to the ACL has become one of the most common athletic injuries and it is the most reconstructed ligament in the human body. In the 1970s, the torn ACL was considered the beginning of a progressive deterioration of the knee that often ended an athlete’s career. However, with the improvement in arthroscopy and sports medicine, many athletes now routinely return to play as soon as four to six months after an injury.
Source of Image: Atlanta’s Resource for Orthopaedic Surgery. https://www.atlantaboneandjoint.com/acltear.html
Figure 1: Diagrammatic representation of Major Knee Ligaments. A – Normal ACL, B – Torn ACL
Further readings
1. Arojuraye SA, Salihu MN, Salahudeen A. Arthroscopic Anterior Cruciate Ligament Reconstruction Learning Curve: Analysis of Operating Time and Clinical Outcomes. J West Afr Coll Surg. 2024 Apr-Jun;14(2):208-211.
2. Alabi IA, Nkanta C, Okoh N, Arojuraye SA and Abbas AD. Functional Outcome of Arthroscopic Reconstruction of Chronic Anterior Cruciate ligament Rupture using Single-bundle Triple-weaved Hamstring Tendons in Northern Nigeria. International Journal of Orthopaedics Sciences 2020; 6(4): 533-538.
3. Leon S, Carol V. David S. Anterior Cruciate Ligament Injuries: Anatomy, Physiology, Biomechanics, and Management. Clin J Sport Med 2012; 22(4): 349 – 355.
4. Douglas WA, Peter RK. Anterior Cruciate Ligament Reconstruction. In: Douglas WJ. Master Techniques in Orthopaedic Surgery; Reconstructive knee Surgery. Lippincott Williams & Wilkins 2008; 3rd Ed, 3: 132 – 153
5. Shelbourne KD, Benner RW, Ringenberg JD, Gray T. Optimal management of posterior cruciate ligament injuries: current perspectives. Orthop Res Rev. 2017;9:13-22
6. Bolgla LA. Gender issues in ACL injury. In: Giangarra CE, Manske RC, eds. Clinical Orthopaedic Rehabilitation: A Team Approach. 4th ed. Philadelphia, PA: Elsevier; 2018:chap 49.
7. Brotzman SB. Anterior cruciate ligament injuries. In: Giangarra CE, Manske RC, eds. Clinical Orthopaedic Rehabilitation: A Team Approach. 4th ed. Philadelphia, PA: Elsevier; 2018:chap 47.
8. Cheung EC, McAllister DR, Petrigliano FA. Anterior cruciate ligament injuries. In: Miller MD, Thompson SR, eds. DeLee, Drez, & Miller’s Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 98.
9. Gokeler A, Dingenen B, Hewett TE. Rehabilitation and return to sport testing after anterior cruciate ligament reconstruction: where are we in 2022? Arthrosc Sports Med Rehabil. 2022;4(1):e77-e82.
10. Kalawadia JV, Guenther D, Irarrázaval S, Fu FH. Anatomy and biomechanics of the anterior cruciate ligament. In: Prodomos CC. The Anterior Cruciate Ligament: Reconstruction and Basic Science. 2nd ed. Philadelphia, PA: Elsevier; 201
8:chap 1.
