The forceps are a double-bladed metal instrument. There have been over 700 variations and modifications to this instrument that have been described over the years and can be broadly classified based on the purpose of its use, Classical forceps, rotational forceps, and specialized forceps used in breech delivery.
Common types include:
- Pipers – used for delivery of after coming head in breech delivery
- Wrigley’s – used as outlet forceps.
- Kielland’s – used for rotational deliveries.
Forceps are generally classified as outlet forceps, low cavity forceps, mid cavity forceps and high cavity forceps. The high cavity forceps delivery is no longer used in clinical practice due to the complications associated with it.
| Type of procedure | Criteria |
| Outlet forceps | 1. Scalp is visible at the introitus without separating labia |
| 2. Fetal skull has reached pelvic floor | |
| 3. Station is > +2 | |
| 4. Sagittal suture is in anteroposterior diameter or right or left occiput anterior or posterior position | |
| 5. Fetal head is at or on perineum | |
| 6. Rotation does not exceed 45° | |
| Low forceps | 1. Leading point of fetal skull is at station 2 cm |
| 2. Fetal skull has not reached the pelvic floor | |
| 3a. Rotation 45° (left or right occiput anterior to occiput anterior, or left or right occiput posterior to occiput posterior) | |
| 3b. Rotation >45° | |
| Mid forceps | Station above +2 cm but head engaged |
| High Forceps | Not included in the classification |
| (American College of Obstetricians and Gynecologists. Operative Vaginal Deliveries. Technical Bulletin No. 196, ACOG, Washington, DC 1994) |

Examples of Obstetrics Delivery forceps. Image courtesy film medical
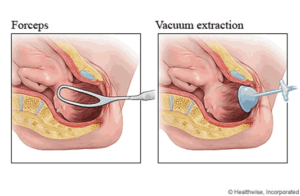
Image courtesy Healthwise incorporated.
Indications for forceps use
Indications for the use of forceps for delivery include maternal exhaustion, prolonged second stage, sickle cell disease in pregnancy, cardiac disease in pregnancy, fetal distress in the second stage of labour, malposition, and delivery of after coming head in breech delivery.
Vacuum (ventouse) device
The ventouse is an instrument that is characterized by the application of a cup to the fetal head via a vacuum device with the aim of achieving vaginal delivery. The device can be manual or automated. The two major types of cups used for the vacuum device are rigid and soft cups. There are more success with the metallic rigid cups, and the automated vacuum when compared with the silastic and manual vacuum. The Kiwi OmniCup is a new single use affordable vacuum that can also be used
Indications for vacuum use
Indications for vacuum use include maternal exhaustion, malposition, fetal distress in the second stage and prolonged second stage.

Metal vacuum cups with its varying sizes: image courtesy IndiaMART

Image courtesy Gynocare Services


