This affects all mucous membrane (oral to anus). Oral mucositis is the most common. Presenta 5-10days following chemotherapy. Mucositis is caused by direct damage of mucosal lining by chemotherapeutic agents or secondary invasion by micro-organisms.
Clinical Presentation(figure 1)
• Burning oral pain.
• Erythema and ulceration.
• Difficulty eating, drinking, talking.
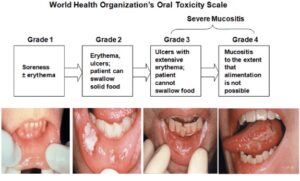
Figure 1 Mucositis. Source: Radiation induced mucositis from Osama et.al.
Diagnosis of mucositis is based on clinical judgement. Oral swab for microscopy, culture and sensitivity should be also taken.
TREATMENT
• Oral debridement eg alcohol help dislodge dried secretion.
• Oral decontamination with antibiotic and antifungal rinsing.
• Pain management.
• Prophylaxis with use of ice chip cryotherapy.
• Low level laser therapy.
INTRODUCTION
This is inflammation of bladder mucosa with oedema and ulceration causing haematuria. Caused by metabolites of cyclophosphamide and Ifosfamide especially acrolein. Acrolein is excreted in urine – it causes oedema, inflammation and necrosis of transitional epithelium with increased contact (Figure 2)
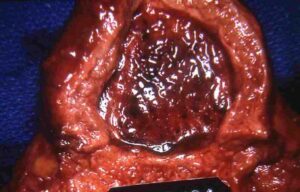
Figure 2: Haemorrhagic CystisImage source: slideshare. Minarcik robbins 2013_ch21-lower_ut
Treatment of Cystitis
• Hyperhydration and continuous bladder irrigation.
• Suprapubic catheterization.
• Platelet transfusion.
• Local instillation of prostaglandin E1, • Alum, Silver nitrate or formalin.
• Bladder resection if intractable.
• Use of Mercapto-ethane sulfonate (mesna) which binds the irritative metabolite, acrolein to produce non-toxic thio-ethers.


