Ectopic pregnancy (EP) is defined as a pregnancy in which the implantation of the embryo occurs outside the uterine cavity, most frequently in one of the two fallopian tubes or, more rarely, in the abdominal cavity. It is a common life-threatening gynecological emergency with significant morbidity and mortality especially in developing countries where majority of the patients present late with ruptured form and hemodynamic instability. During the first three months of pregnancy, EP is the leading cause of maternal death in industrialized countries, and possibly the second most frequent cause in developing countries (after abortion complications). Most ectopic pregnancies occur in women aged 25-34 years.
The commonest site of Ectopic Pregnancies is the fallopian tube which accounts for 95 percent of ectopic pregnancies: 55 percent in the ampulla; 20 percent in the isthmus; 17 percent in the fimbria; 2-4 percent in the interstitial. Other sites are the cornual part of the uterus, abdominal cavity, ovary, cervix, broad ligament and rudimentary horn. The right tube is more frequently affected probably as a result of appendicular inflammation.
The incidence of ectopic pregnancy varies among different countries, in same geographical region depending on the prevailing risk factors. In Nigeria, it ranges between 1.1-3.8% of deliveries compared to a rate of 11 per 1000 pregnancies in the UK and 19.6 per 1000 pregnancies in North America. There has been a gradual increase over the years, probably as a true reflection of the larger number of cases in the population or because of improved sensitivity of diagnostic tests for ectopic pregnancy.
Aetiological factors include history of multiple sexual partners and pelvic infections particularly with Chlamydia infection6, as well as history of previous ectopic pregnancy, IUCD or sterilization failure with a reported risk of 7 per 1000 in patients with pregnancies following sterilization procedures.Other associated aetiological factors include previous pelvic or tubal surgery, gross pelvic pathology such as endometriosis, congenital abnormalities of the tubes such as diverticula, accessory Ostia, hypoplasia, in utero diethylstilbestrol (DES) exposure.A history of previous induced abortion or infertility and current smoking increase risk.Contraceptive use reduces the annual risk for intrauterine and ectopic pregnancy; however, previous intrauterine device use may increase risk.Other causes include oral progestin-only contraceptive, pelvic adhesion and in vitro fertilization and embryo transfer.
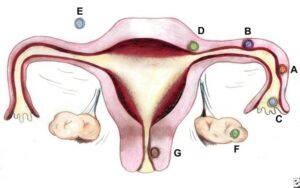
Sites and frequencies of ectopic pregnancy. By Donna M. Peretin, RN. (A) Ampullary (B) Isthmic (C) Fimbrial (D) Cornual/Interstitial; (E) Abdominal(F) Ovarian; and (G) Cervical.

Ectopic pregnancy (EP) is defined as a pregnancy in which the implantation of the embryo occurs outside the uterine cavity, most frequently in one of the two fallopian tubes or, more rarely, in the abdominal cavity. It is a common life-threatening gynecological emergency with significant morbidity and mortality especially in developing countries where majority of the patients present late with ruptured form and hemodynamic instability. During the first three months of pregnancy, EP is the leading cause of maternal death in industrialized countries, and possibly the second most frequent cause in developing countries (after abortion complications). Most ectopic pregnancies occur in women aged 25-34 years.
The commonest site of Ectopic Pregnancies is the fallopian tube which accounts for 95 percent of ectopic pregnancies: 55 percent in the ampulla; 20 percent in the isthmus; 17 percent in the fimbria; 2-4 percent in the interstitial. Other sites are the cornual part of the uterus, abdominal cavity, ovary, cervix, broad ligament and rudimentary horn. The right tube is more frequently affected probably as a result of appendicular inflammation.
The incidence of ectopic pregnancy varies among different countries, in same geographical region depending on the prevailing risk factors. In Nigeria, it ranges between 1.1-3.8% of deliveries compared to a rate of 11 per 1000 pregnancies in the UK and 19.6 per 1000 pregnancies in North America. There has been a gradual increase over the years, probably as a true reflection of the larger number of cases in the population or because of improved sensitivity of diagnostic tests for ectopic pregnancy.
Aetiological factors include history of multiple sexual partners and pelvic infections particularly with Chlamydia infection6, as well as history of previous ectopic pregnancy, IUCD or sterilization failure with a reported risk of 7 per 1000 in patients with pregnancies following sterilization procedures.Other associated aetiological factors include previous pelvic or tubal surgery, gross pelvic pathology such as endometriosis, congenital abnormalities of the tubes such as diverticula, accessory Ostia, hypoplasia, in utero diethylstilbestrol (DES) exposure.A history of previous induced abortion or infertility and current smoking increase risk.Contraceptive use reduces the annual risk for intrauterine and ectopic pregnancy; however, previous intrauterine device use may increase risk.Other causes include oral progestin-only contraceptive, pelvic adhesion and in vitro fertilization and embryo transfer.
Sites and frequencies of ectopic pregnancy. By Donna M. Peretin, RN. (A) Ampullary (B) Isthmic (C) Fimbrial (D) Cornual/Interstitial; (E) Abdominal(F) Ovarian; and (G) Cervical.
- Audu LR, Ekele BA. A ten year review of maternal mortality in Sokoto, Northern Nigeria. WAJM 2002; 21(1): 74 – 76.
- Ola ER, Imosemi DO, Egwatu J I, Abudu O.O. Ectopic Pregnancy: Lagos University Teaching Hospital experience over a five-year period, Nig Qt J Hosp Med 1990; 9(2):100 – 103.
- Mark AD, John AR. Ectopic pregnancy In: Te Lindes operative Monga A. (ed.) Disorders of early pregnancy. Tenth edition. John AR, Howard WJ. (eds.) Lippincott Williams and Wilkins; Philadelphia. 2008 Pp. 798-824.
- Oloyode OAO, Lamina MA, Odusuga OL, Adetuye PO, Olatunji AO, Fakoya TA, Sule-Odu AO, Jagun OE. Ectopic Pregnancy in Sagamu, a 12 year review. Trop J Obstet Gynaecol, 2002; 19(2) 34.
- Olatunbosun OA., Okonofua FE: Ectopic pregnancy. The African Experience –Postgraduate Doctor – Africa. 1996; 8(3): Pp. 74-78.
- Davor J. Ectopic pregnancy. In: Edmonds DK (ed.) Dewhurst’s textbook of Obstetrics and Gynaecology for Postgraduates. 7th ed. Oxford Blackwell Scientific Publications, Oxford. 2007 : Pp. 106-16.
- RCOG 2004. Why mothers die 2000-2002. The sixth report of the confidential enquiry into maternal deaths in the United Kingdom. 2000-2002. London: RCOG press.
- Orji EO, Fasubaa OB, Adeyemi B, Dare FO, Onwudiegwu U, Ogunniyi SO. Mortality and morbidity associated with misdiagnosis of ectopic pregnancy in a defined Nigerian population. J Obstet Gynaecol. 2002 Sep; 22(5): Pp. 548-50.
- Swende TZ, Jogo AA. Ruptured tubal pregnancy in markurdi, north central Nigeria. Acta Obstet Gynecol Scand. 2008. Jan-Mar; 17(1): Pp. 75-7.
- Onwuhafua PI, Onwuhafua A, Adesiyun GA, Adze J. Ectopic pregnancies at the Ahmadu Bello University Teaching Hospital, Kaduna, Northern Nigeria. Tropical Journal of Obstetrics and Gynaecology 2001; 18(2): 82 – 86.
- Hajenius PJ, Mol BWJ, Bossuyi PMM, Ankum WM, Van der Veen F. Interventions for tubal ectopic pregnancy (Cochrane Review). In: The Cochrane Library, Issue 2 2003. Oxford: Update software\
- Patrick Thonnean et al. Ectopic pregnancy in Conakry, Guinea, Bull World Health Organ vol. 80 no. 5 2002
- Verema T Valley. Ectopic pregnancy. eMedicine Specialities 2005.
- Anne-Marie L, Beth Potter. Diagnosis and management of ectopic pregnancy. Am Fam physician. 2005; 72(9): 1707 – 1714.
- Bouyer J, Job-Spiral N, Pouly JL 1996, Fertility after ectopic pregnancy- results of the first three years of the Auvergne register. Contracept Fertil Sex 24, Pp. 475-81

Background
Ectopic pregnancy (EP) is defined as a pregnancy in which the implantation of the embryo occurs outside the uterine cavity, most frequently in one of the two fallopian tubes or, more rarely, in the abdominal cavity. It is a common life-threatening gynecological emergency with significant morbidity and mortality especially in developing countries where majority of the patients present late with ruptured form and hemodynamic instability. During the first three months of pregnancy, EP is the leading cause of maternal death in industrialized countries, and possibly the second most frequent cause in developing countries (after abortion complications). Most ectopic pregnancies occur in women aged 25-34 years.
The commonest site of Ectopic Pregnancies is the fallopian tube which accounts for 95 percent of ectopic pregnancies: 55 percent in the ampulla; 20 percent in the isthmus; 17 percent in the fimbria; 2-4 percent in the interstitial. Other sites are the cornual part of the uterus, abdominal cavity, ovary, cervix, broad ligament and rudimentary horn. The right tube is more frequently affected probably as a result of appendicular inflammation.
The incidence of ectopic pregnancy varies among different countries, in same geographical region depending on the prevailing risk factors. In Nigeria, it ranges between 1.1-3.8% of deliveries compared to a rate of 11 per 1000 pregnancies in the UK and 19.6 per 1000 pregnancies in North America. There has been a gradual increase over the years, probably as a true reflection of the larger number of cases in the population or because of improved sensitivity of diagnostic tests for ectopic pregnancy.
Aetiological factors include history of multiple sexual partners and pelvic infections particularly with Chlamydia infection6, as well as history of previous ectopic pregnancy, IUCD or sterilization failure with a reported risk of 7 per 1000 in patients with pregnancies following sterilization procedures.Other associated aetiological factors include previous pelvic or tubal surgery, gross pelvic pathology such as endometriosis, congenital abnormalities of the tubes such as diverticula, accessory Ostia, hypoplasia, in utero diethylstilbestrol (DES) exposure.A history of previous induced abortion or infertility and current smoking increase risk.Contraceptive use reduces the annual risk for intrauterine and ectopic pregnancy; however, previous intrauterine device use may increase risk.Other causes include oral progestin-only contraceptive, pelvic adhesion and in vitro fertilization and embryo transfer.
Sites and frequencies of ectopic pregnancy. By Donna M. Peretin, RN. (A) Ampullary (B) Isthmic (C) Fimbrial (D) Cornual/Interstitial; (E) Abdominal(F) Ovarian; and (G) Cervical.
Further readings
- Audu LR, Ekele BA. A ten year review of maternal mortality in Sokoto, Northern Nigeria. WAJM 2002; 21(1): 74 – 76.
- Ola ER, Imosemi DO, Egwatu J I, Abudu O.O. Ectopic Pregnancy: Lagos University Teaching Hospital experience over a five-year period, Nig Qt J Hosp Med 1990; 9(2):100 – 103.
- Mark AD, John AR. Ectopic pregnancy In: Te Lindes operative Monga A. (ed.) Disorders of early pregnancy. Tenth edition. John AR, Howard WJ. (eds.) Lippincott Williams and Wilkins; Philadelphia. 2008 Pp. 798-824.
- Oloyode OAO, Lamina MA, Odusuga OL, Adetuye PO, Olatunji AO, Fakoya TA, Sule-Odu AO, Jagun OE. Ectopic Pregnancy in Sagamu, a 12 year review. Trop J Obstet Gynaecol, 2002; 19(2) 34.
- Olatunbosun OA., Okonofua FE: Ectopic pregnancy. The African Experience –Postgraduate Doctor – Africa. 1996; 8(3): Pp. 74-78.
- Davor J. Ectopic pregnancy. In: Edmonds DK (ed.) Dewhurst’s textbook of Obstetrics and Gynaecology for Postgraduates. 7th ed. Oxford Blackwell Scientific Publications, Oxford. 2007 : Pp. 106-16.
- RCOG 2004. Why mothers die 2000-2002. The sixth report of the confidential enquiry into maternal deaths in the United Kingdom. 2000-2002. London: RCOG press.
- Orji EO, Fasubaa OB, Adeyemi B, Dare FO, Onwudiegwu U, Ogunniyi SO. Mortality and morbidity associated with misdiagnosis of ectopic pregnancy in a defined Nigerian population. J Obstet Gynaecol. 2002 Sep; 22(5): Pp. 548-50.
- Swende TZ, Jogo AA. Ruptured tubal pregnancy in markurdi, north central Nigeria. Acta Obstet Gynecol Scand. 2008. Jan-Mar; 17(1): Pp. 75-7.
- Onwuhafua PI, Onwuhafua A, Adesiyun GA, Adze J. Ectopic pregnancies at the Ahmadu Bello University Teaching Hospital, Kaduna, Northern Nigeria. Tropical Journal of Obstetrics and Gynaecology 2001; 18(2): 82 – 86.
- Hajenius PJ, Mol BWJ, Bossuyi PMM, Ankum WM, Van der Veen F. Interventions for tubal ectopic pregnancy (Cochrane Review). In: The Cochrane Library, Issue 2 2003. Oxford: Update software\
- Patrick Thonnean et al. Ectopic pregnancy in Conakry, Guinea, Bull World Health Organ vol. 80 no. 5 2002
- Verema T Valley. Ectopic pregnancy. eMedicine Specialities 2005.
- Anne-Marie L, Beth Potter. Diagnosis and management of ectopic pregnancy. Am Fam physician. 2005; 72(9): 1707 – 1714.
- Bouyer J, Job-Spiral N, Pouly JL 1996, Fertility after ectopic pregnancy- results of the first three years of the Auvergne register. Contracept Fertil Sex 24, Pp. 475-81
