Clubfoot is the most common musculoskeletal deformity with a global incidence of about 1:1000 live births. In it, the foot is turned inward and downward. Literature has it that more than 80% of clubfoot cases are found in the LMICs for reasons that are not entirely clear, though many have assumed that the reason is not unrelated to the higher birth rates at LMICs.

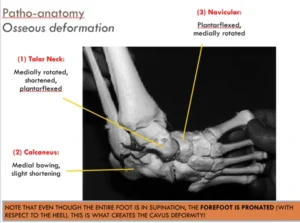
Patho-anatomy of Clubfoot
Clubfoot, also known as Congenital Talipes EquinoVarus (CTEV), comprises 4 major deformities remembered as C-A-V-E meaning cavus, adductus, varus, and equinus. While the first two occur at the midfoot, the last two are seen at the hindfoot. The cavus is a high longitudinal medial arch and is due to the first ray of the foot falling off the plane with the other metatarsals. The adductus is due to the navicular which is turned medially causing the forefoot to be turned inwards while the lateral rotation of the calcaneum causing a heel varus.
Pirani score is used to assess the severity of deformity, plan the treatment and monitor the progress. It is a 6-point scoring system that measures six parameters that are scored 0, 0.5 and 1 depending on whether the deformity was absent, moderate or severe in appearance. The six parameters are divided into the MidFoot Contracture Score (MCFS) and the HindFoot Contracture Score (HFCS) with three parameters each.
The components of the MFCS are the presence of a medial crease, the curvature of the lateral border and the prominence of the lateral head of Talus. The HFCS has the presence of a posterior crease, the emptiness of the heel and the posterior crease.

Management of Clubfoot
The globally accepted standard of clubfoot care today is the minimally invasive Ponseti method. Named after Ignacio Ponseti, the Spanish surgeon at the University of Iowa who popularized it, Ponseti treatment consists of the sequential manipulation and casting, percutaneous tendo Achilles tenotomy and then, foot abduction bracing.
The manipulation is done weekly, and each stretch is held with a cast. The first manipulation corrects cavus by lifting the first ray to be on the same plane as the other metatarsals. This elevates the first ray and supinates it to be in line with the rest of the foot. To the layman, it seems like the foot became worse in appearance. Thereafter, the adductus is gradually corrected, to gain more abduction. The varus, through the process of kinematic coupling, corrects passively with the correction of the adductus. The cast applied after each correction extends from the toe to the groin and has the knee flexed to 90 degrees.

The last correction is that of the residual equinus and this is done with the percutaneous tendo Achilles tenotomy. A size 15 blade is preferably used, though some may use the Beaver blade or size 11 blade. After the tenotomy, the cast is left for 2-3 weeks and thereafter the foot-abduction-brace wear commenced.
The foot abduction brace marks the maintenance phase of the Ponseti treatment. At the initial stage, the child wears it full time (23 hours a day) except when he/she is taking a bath. Thereafter, nap times and nighttime wear are advocated till the age of 5 years. Noncompliance with the brace wear protocol is incriminated to be the reason for most relapses and recurrences following correction of the clubfoot deformity using the Ponseti technique. Parents and caregivers need to be educated and every opportunity to talk to them should be seized to enhance their cooperation and adherence to the protocol.

For complex clubfoot cases and recurrences, some sort of surgery may be required, and unless one is competent, a referral to a paediatric orthopaedic surgeon may be necessary.
Conclusion
Clubfoot is the most common musculoskeletal deformity worldwide, with a higher prevalence in low- and middle-income countries. The condition is characterized by four main deformities: cavus, adductus, varus, and equinus. This is assessed using the Pirani scoring system. The Ponseti method, which includes manipulation, casting, tenotomy, and bracing, is the global standard for treatment. Consistent use of foot abduction braces is essential to prevent relapses after correction. Complex or recurrent cases may require surgical intervention or referral to a pediatric orthopaedic specialist.
Author’s reflections:
People have also done the accelerated Ponseti and others, a two-weekly cast. I would rather prefer that people learnt the correct version of the original Ponseti before they start to modify.
Foot abduction braces are used to maintain the correction. Ortho shoes are not encouraged.

Clubfoot is the most common musculoskeletal deformity with a global incidence of about 1:1000 live births. In it, the foot is turned inward and downward. Literature has it that more than 80% of clubfoot cases are found in the LMICs for reasons that are not entirely clear, though many have assumed that the reason is not unrelated to the higher birth rates at LMICs.
- Ponseti, I. V. and E. N. Smoley (2009). “The classic: congenital club foot: the results of treatment. 1963.” Clin Orthop Relat Res 467(5): 1133–1145.
- Smythe, T., R. M. Owen, A. Aspden, J. Everhart, E. Abera, P. Amaraegbulam, R. Flores, L. Valdez and C. Lavy (2025). “Global clubfoot treatment in 2023: an overview of advances and outcomes.” BMJ Glob Health 10(3).
- Staheli, L. (2009). Clubfoot: Ponseti management, Global HELP Organization.

Background
Clubfoot is the most common musculoskeletal deformity with a global incidence of about 1:1000 live births. In it, the foot is turned inward and downward. Literature has it that more than 80% of clubfoot cases are found in the LMICs for reasons that are not entirely clear, though many have assumed that the reason is not unrelated to the higher birth rates at LMICs.
Further readings
- Ponseti, I. V. and E. N. Smoley (2009). “The classic: congenital club foot: the results of treatment. 1963.” Clin Orthop Relat Res 467(5): 1133–1145.
- Smythe, T., R. M. Owen, A. Aspden, J. Everhart, E. Abera, P. Amaraegbulam, R. Flores, L. Valdez and C. Lavy (2025). “Global clubfoot treatment in 2023: an overview of advances and outcomes.” BMJ Glob Health 10(3).
- Staheli, L. (2009). Clubfoot: Ponseti management, Global HELP Organization.
